Eating disorders (EDs) are associated with elevated all-cause mortality, with suicide cited as the second leading cause of death among individuals with EDs. Evidence suggests that individuals with anorexia nervosa are 18 times, and those with bulimia nervosa seven times more likely to die by suicide, relative to gender- and age-matched comparison groups. Limited research has focused on why people with EDs experience such high rates of suicidality. The study aims to gather perspectives from people with lived experience of an ED and clinicians working with EDs to understand suicidality among people with EDs.
Methods
Using a qualitative design, we conducted semi-structured interviews with people with lived experience of an ED (n?=?30), and clinicians who work with people with EDs (n?=?19). Participants with lived experience presented with a range of EDs. Clinicians worked across a range of service settings as well as adolescent and adult services. We used a multi-perspective reflexive thematic analysis to code the data and generate the themes.
Results
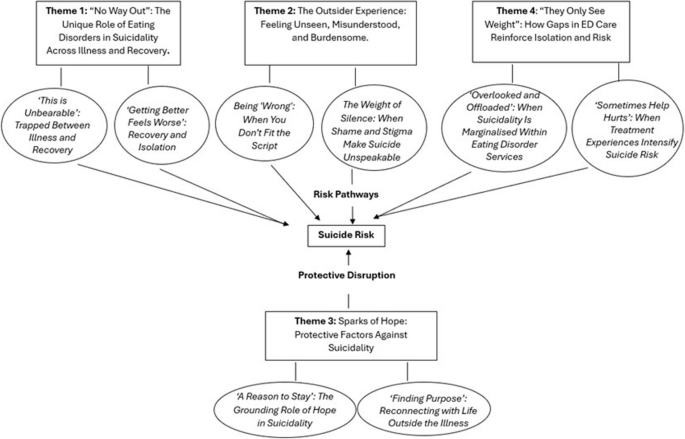
Key themes identified include ‘no way out’: the unique role of eating disorders in suicidality across illness and recovery, the outsider experience: feeling unseen, misunderstood, and burdensome, sparks of hope: protective Factors against suicidality, and ‘they only see weight’: how gaps in ED care reinforce isolation and risk. These findings underscore the complex and multifaceted reasons why people with EDs are at risk of suicide, acknowledging the unique risk factors associated with the illness itself as well as the various risk periods that affect those with EDs.
Conclusions
The results are novel and illuminate psychological processes that are not currently incorporated within existing theoretical models of suicide, indicating that prevailing frameworks may lack the specificity or sensitivity required to account for the distinctive experiences of individuals with EDs. Consequently, these findings provide preliminary evidence to inform the development of a more nuanced theoretical model of suicidality specific to this population. Moreover, they suggest potential targets for intervention and highlight the need to critically evaluate treatment approaches that prioritise rapid symptom remission, which may, at times, exceed individuals’ psychological capacity to cope.
Eating disorders (EDs), such as anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), avoidant/restrictive food intake disorder (ARFID), and otherwise specified feeding and eating disorder (OSFED), are a major global health concern, with rising incidence rates internationally since the COVID-19 pandemic [1]. While reported mortality rates have decreased over time [2], EDs remain associated with elevated all-cause mortality risk [3, 4]. Suicide is a leading cause of death among people with EDs, and suicidal behaviour and self-harm are elevated in this group relative to the general population [5]. Studies have found that people with AN are 18 times more likely to die by suicide, and those with BN are seven times more likely to die by suicide, relative to gender and age-matched comparison groups [5]. Figures show that up to a third of people with lived experience of EDs, across the range of diagnoses, have attempted suicide [6]. Furthermore, studies have shown that people with EDs have significantly higher rates of both non-suicidal self-injury (NSSI) and suicidal ideation compared to healthy and psychiatric control groups [7,8,9,10,11].
Although previous literature has consistently demonstrated that individuals with EDs are at heightened risk of suicide, limited research explores the underlying reasons for the elevated rates of suicidal ideation and behaviour in this population. A meta-analysis found that having an ED alone does not fully explain the high suicide rates observed in this population [12]. The findings indicate that disordered eating symptoms are weak predictors of suicide attempts and do not predict death by suicide.
Various explanations for the co-occurrence of suicidality and EDs have been suggested. Previous explanations explored this link using existing psychological theories of suicidality, such as the Interpersonal Theory of Suicide (IPTS) [13]. The IPTS [13] is one of the most influential theories in suicidality and proposes that individuals are at risk of suicide if they simultaneously experience three factors: thwarted belonging (e.g. the feeling of being alienated from others), perceived burdensomeness (e.g. the feeling of being a burden or liability to others and belief that others would benefit from one’s death) and Acquired Capability for Suicide (ACS) (e.g. lowered fearlessness about death and an elevated tolerance of physical pain resulting from habituation to painful and/or provocative events) [13]. Reviews of research findings suggest this theoretical framework does not fully explain the complex nature of EDs increased risk of suicide [14]. Reviews have identified a wide range of factors, including illness severity, co-occurring psychiatric illnesses (including borderline personality disorder and substance abuse), excessive exercise, and alexithymia, as possible risk factors explaining the ED-suicide link [15]. These exemplify the complex challenges faced by suicide theories in accounting for the ED–suicide link [14].
Overall, the literature highlights that EDs are consistently associated with elevated rates of suicidality, including suicidal ideation, attempts, and completed suicide. However, the nature of this relationship remains poorly understood. While numerous studies have demonstrated a strong link between EDs and suicidality, it is unclear to what extent EDs directly contribute to increased suicide risk or whether this association is influenced by other psychological, biological, or social factors. Existing theoretical models of suicide do not fully account for the unique experiences and risk mechanisms specific to individuals with EDs. Therefore, further research is needed to elucidate the pathways through which EDs may elevate suicidality, which could inform the development of targeted interventions and refined theoretical frameworks.
Qualitative research can support such development by exploring novel themes that intertwine across theories and thus provide insights into the driving factors for suicidality in this group, as exemplified by qualitative work in the area of self-harm [16]. To the authors’ knowledge, there are no studies to date that utilise a qualitative interview methodology to explore suicidality risk for people with EDs.
Aim
The purpose of this research was to develop a more detailed and nuanced understanding of the inter-relationship between EDs and increased risk of suicidality. We aimed to do this through exploring the experiences and perspectives of people living with an ED and healthcare participants who work with EDs. By including both perspectives, we aimed to provide a range of diverse perspectives on this issue to further inform treatment interventions.
#James Donaldson notes: Welcome to the “next chapter” of my life… being a voice and an advocate for #mentalhealthawarenessandsuicideprevention, especially pertaining to our younger generation of students and student-athletes. Getting men to speak up and reach out for help and assistance is one of my passions. Us men need to not suffer in silence or drown our sorrows in alcohol, hang out at bars and strip joints, or get involved with drug use. Having gone through a recent bout of #depression and #suicidalthoughts myself, I realize now, that I can make a huge difference in the lives of so many by sharing my story, and by sharing various resources I come across as I work in this space.#http://bit.ly/JamesMentalHealthArticle Find out more about the work I do on my 501c3 non-profit foundation website www.yourgiftoflife.org Order your copy of James Donaldson’s latest book, #CelebratingYourGiftofLife: From The Verge of Suicide to a Life of Purpose and Joy
We used an exploratory qualitative approach and conducted semi-structured interviews with people with lived experience of EDs and suicidality, and healthcare professionals who have experience working with individuals with EDs.
Sample selection, eligibility, and recruitment
The study recruited two groups of participants: those with lived experience of an ED and suicidality (lived experience participants), and those who had experience working with people with EDs (healthcare participants). Inclusion and exclusion criteria are described in Table 1.Table 1 Eligibility criteria for participants
The study was advertised via social media platforms (e.g. personal and institutional X accounts), the MQ Participate platform (a platform that connects researchers who are looking for participants for their research), and via a range of healthcare professional and charity networks, e.g. First Steps ED. Advertisement posters included information about the study, e.g. the study title and aim (‘we are recruiting for a new study entitled ‘Why are people with eating disorders at high risk of suicide?’ that we would like to invite you to take part in. This project will help us to better understand why people with eating disorders are at a high risk of suicide.’), inclusion criteria, and a link to a Microsoft Forms screening questionnaire in which participants were provided with additional information about study participation (e.g. ‘taking part in this study would involve having a 1–2-1 interview with a member of our research team about your experiences and views on this topic, which may involve asking some sensitive questions about suicide, self-harm, eating disorders’) followed by a list of questions to register their interest in participation, their contact details, and screening questions to confirm eligibility. Eligible participants were sent the relevant Participant Information Sheet (PIS), with separate versions for lived experience and healthcare participants. Participants were asked to read the PIS and consider if they wished to participate and were given time to ask any questions about the study. Interested participants were placed on a waiting list for an interview date. Due to high interest, quota sampling was used to ensure diversity of participants. Quota sampling is a method for selecting numbers of subjects to represent the conditions to be studied with the goal of inclusion of people who may be underrepresented by convenience or purposeful sampling techniques [17]. For those with lived experience of an ED, we considered diversity in recruitment related to key demographics such as gender (to ensure the inclusion of male, non-binary and trans people), a range of ethnic and cultural backgrounds, those with neurodivergence, a range of ED diagnoses, and a range of treatment experiences (including those with no experience of treatment, community only and inpatient treatment experience). For healthcare professionals, we aimed to include a diverse range of participants from a range of disciplines, care settings, and years of experience working with ED. To ensure diversity, we used targeted recruitment (e.g. contacting organisations such as male ED charities to circulate recruitment materials via their networks) and kept an ongoing record of the key demographics and backgrounds of people we interviewed, reviewing this routinely to ensure we were accessing a range of experiences and views from a diverse group of participants. Ineligible participants and those who were not selected for interview due to high interest were sent an email thanking them for their interest.
Procedure
Semi-structured individual research interviews were conducted between December 2023 and April 2024. Drawing on existing literature, semi-structured interview topic guides were developed in collaboration with our Lived Experience Advisory Panel (LEAP). Guides consisted of key questions on topics related to EDs and suicidality, including asking about their experience of this, why they felt people with EDs were at high risk of suicide, and what protective factors against suicidality exist for people with EDs. Questions included asking about participants’ experience of having an ED and suicidality or working with people with EDs who experienced suicidality, exploring if participants’ view on the ED-suicide link (e.g. ‘thinking about your own experiences, do you think eating disorders are linked to high rates of suicidality, and why/why not?’, ‘why do you think people with EDs might experience suicidality?’), what factors may be associated with suicide risk for people with EDs, and what protective factors help people who have EDs and experience these risks/suicidality. These topic guides were used as a flexible tool to direct participants towards the key research questions.
Participants were invited to take part in an interview with the lead author (UF) at a time and date that was convenient to them, either remotely or within the university. Prior to the interview, participants were provided with a copy of the PIS and consent form that would be used on the day of the interview. Eligible participants were sent copies of the participant information sheet at least 24 h before the interview. Due to the sensitive nature of the interview, the lived experience participants were asked to provide contact details for a family member or friend that the research team could contact if they had concerns for the participant’s safety during the interview.
Interviews were scheduled for 1 h with an additional 15 min before and after to obtain informed consent and answer any questions. Participation was voluntary and participants were free to withdraw at any time. Informed consent was obtained from all participants prior to the interview, either in written form or verbally recorded. Interviews were audio-recorded and saved to an encrypted server. To thank participants for their time and sharing their experiences, we offered a £25 voucher following the interview. Audio recordings were transcribed verbatim by an external company, and the research team checked the transcripts for accuracy and pseudonymised data. All transcripts were allocated a unique ID number and imported to NVivo [18] for analysis.
Philosophical positioning and analytic approach
This study employed reflexive thematic analysis (RTA) [19], underpinned by a critical realist perspective. This position recognises that participants’ experiences are real and meaningful, while also shaped by wider social, cultural, and relational contexts [20]. The analysis aimed to explore not only what participants reported, but how they made sense of their experiences.
Interpretation was informed by existing literature on EDs, suicidality, and mental health, which helped contextualise findings and highlight meaningful patterns. Themes were viewed as constructed through the analytic process, shaped by the studies’ questions, and researchers’ values and interpretive lens.
Data analysis
Interviews were recorded, transcribed, and anonymised prior to coding. We undertook a multi-perspective RTA following the phases and definitions outlined by Braun and Clarke [21]. The aim of this data analysis was to develop an understanding of participants’ experiences and beliefs around if and why suicide risk is high among people with EDs, and the risk and protective factors associated with suicide among people with EDs. The analysis used an inductive approach to the data coding in which themes were selected based on the data collected rather than to fit pre-existing codes. This method enabled deep exploration of the data due to its flexibility, which allowed themes to highlight the similarities and differences between differing participant groups involved in the research. Guided by the overarching study aim, members of the research team (authors UF, SK, AM, and MH) read and re-read the interview transcripts to identify preliminary codes. All transcripts were double coded to help check interpretations against the data. Codes were defined as a single idea identifying what is of interest in the data. A line-by-line coding approach was used to ensure that data across the entire interview was coded to avoid missing out on key points. During coding, lived experience data and healthcare professionals’ data were coded as separate datasets. Following initial coding, each data set was reviewed and related codes were sorted, grouped, and labelled as preliminary themes, which are central concepts that capture and summarise the core point of a meaningful pattern in the data. The two data sets’ codes and developing themes were compared to view if the themes overlapped and diverged. With a single dataset combining the two participant group analyses, themes were reviewed, discussed, and revised within the wider research team to ensure they were capturing themes relevant across the data, that captured both perspectives meaningfully as well as acknowledging where there were diverging views. To improve validity, transparency, and quality, we repeatedly reviewed the themes within the wider study group until a consensus was reached that a theoretically sufficient account had been created, and no new concepts were being generated. Data extracts illustrate each theme and key analytic points.
Ethics
Ethical approval was granted by the King’s College London Health Faculties (Blue) Research Ethics Subcommittee (reference number HR/DP-22/23–38,891).
Patient and public involvement
The study methodology, design, and data collection, including the development of the topic guide, were developed by the team in collaboration with a researcher with lived experience of an ED and suicidality. All interviews were conducted and analysed by a member of the research team with lived experience of an ED. In addition, we recruited and facilitated a ten-member LEAP. This group was made up of individuals with experience of a range of EDs and suicidality. Members were of diverse ethnic backgrounds and included eight women, one man, and one non-binary person. The panel was chaired by the lead author (UF), and they provided guidance and support for the research team across the whole research study, including during the development of the interview schedule, practice interviews prior to data collection, and supported the analysis and interpretation of the data, as well as the writing of the final paper. The LEAP met at least twice a year for 2 h, with more frequent meetings during the study’s data collection period and during interpretation and writing up of the findings. Due to the personal and sensitive nature of the study, additional one-to-one meetings were offered by the lead author with LEAP panel members to provide a safe space to discuss the study or issue that the panel brought up around this topic. Participants in the LEAP were reimbursed for their time and contributions.
Reflexivity and positionality
As researchers conducting this qualitative study, we acknowledge that our individual backgrounds, experiences, and perspectives inevitably influenced the research process and outcomes [22]. In qualitative analysis, the researcher’s subjective sociocultural, political, and ideological positionings are understood to shape the production of meaning in unique ways [19]. Reflexivity involves a critical examination of how such positionality influences the research process, thereby enhancing both rigour and transparency [23, 24].
Our team comprised researchers (including qualitative and quantitative-focused researchers), clinicians, and individuals with lived experience of EDs and suicidality, each bringing unique insights and potential biases to the study. The lead author is a Lived Experience (LE) researcher with lived experience associated with the study topic. Whilst their LE ensures valuable insights, they do not have a definitive voice on EDs or suicidality because, as a white researcher, their viewpoint is already centred. While the inclusion of LE has provided the authors with a deep understanding of EDs and suicidality, it also introduced the possibility of over-identifying with participants’ experiences, potentially leading to biases in data interpretation. Thus, the lead author engaged in reflexivity by completing a diary and reflecting with LE coauthors, LE colleagues and supervisors. Additionally, the lead author’s position as an LE researcher offered valuable insider perspectives but also posed challenges in maintaining objectivity. The team were mindful of the potential for personal experiences to shape the research findings and made concerted efforts to bracket these influences during data analysis through open and reflexive discussion during coding meetings and within the lead author’s supervision.
Consideration of positionality related to authors’ clinician backgrounds was also considered during these meetings. The team collectively engaged in reflexive discussions to explore how our identities and experiences shaped our interpretations. We recognised that our diverse perspectives enriched the analysis but also necessitated ongoing self-awareness to ensure the credibility and trustworthiness of our findings.
Results
Participant characteristics
A total of 49 interviews were conducted with lived experience participants (n?=?30) and healthcare participants (n?=?19). Interviews lasted an average of 52 min.
The majority of lived experience participants were female, White, from England, with experience of AN. Most participants had experience of depression and self-harm alongside their ED and had experience of treatment services (n?=?25). Most participants reported a disability (n?=?17) with mental health conditions and neurodiversity cited as the main disability experienced by participants. See Table 2 for more details of participants’ characteristics.Table 2 Lived experience participants demographics (n?=?30)
For healthcare participants, the majority were females, from a White ethnic background, and all were working in England. A range of professional roles were held by participants, with mental health nursing as the most frequently held role (n?=?5). The majority of participants held roles in a National Health Service (NHS) service (n?=?12), across a range of community settings as well as specialist roles in inpatient services and children and young persons’ services. Six participants identified as having lived experience of an ED as well as their clinician role. See Table 3 for more detail of participants’ characteristics. Two participants worked for the same national charity in different support service roles. All other participants were recruited from different services across England, with no other participants recruited from the same NHS Trust or service.Table 3 Healthcare participants demographics (n?=?19)
Four themes were developed, each with explanatory subthemes outlined in Fig. 1.
Fig. 1
Theme 1—‘no way out’: the unique role of eating disorders in suicidality across illness and recovery
This theme explores how, for people with EDs, suicidality was deeply shaped by the experience of being trapped both within the illness and in the process of trying to recover from it. Suicide was frequently described as a perceived escape from this unliveable bind; a response not to a moment of crisis but to the chronic sense of entrapment the ED produced. This pervasive feeling of having ‘no way out’ was consistently linked to increased suicidal thoughts, feelings, and behaviours. This theme demonstrates how suicidality was not limited to moments of acute illness or a reaction to treatment pressures alone, but rather, emerged from the deeper structure of how the ED shaped identity, agency, and perceived future.
The two subthemes below exemplify these experiences and explore how the unique illness experience of having an ED is closely linked to increased suicidality for individuals.
a‘This is unbearable’: trapped between illness and recoveryParticipants with both lived experience and clinical perspectives described the day-to-day reality of living with an ED as emotionally and physically exhausting, and often painful. Participants described the lived experience as feeling like an ‘ongoing fight’, one that is ‘relentless’ and takes over every waking minute of the day. Living with an ED was frequently described as emotionally and physically exhausting, with several participants likening it to a chronic fight for survival; a fight that sometimes felt unbearable leading to suicidal thoughts as a means of escape.It became this horrible, endless, relentless journey… you just think, what if this is what life is going to be? I’m not signed up for it. II can’t do this, I’ll never be happy and be myself again so I would rather just not be here. (PT17, lived experience)This quote reflects a sense of existential hopelessness. Reflecting the wording of other participants, the experience of the ED as ‘relentless’ speaks to the ongoing toll that the illness has on individuals. Suicidality thus appears not as a desire to die, but as a response to the perceived impossibility of living like this indefinitely.However, even amid this suffering, the alternative of recovery did not necessarily represent safety or relief as it did not represent an obvious escape, but rather a leap into the unknown, where pain persisted and coping structures vanished. As represented below, the ED was not only a source of harm but also a tool for survival. Its removal therefore felt threatening.I’m not allowed to use that [the ED] as a coping mechanism anymore, so what do I do? I haven’t been given anything else… the only thing I know that works is starving myself… so what is there? (PT04, lived experience)Rather than feeling liberated, the absence of the ED could evoke feelings of exposure, loss, and abandonment. The participant articulates a gap: a space where the ED used to be, but which remains unfilled by alternative support. From this position, recovery can feel like an emotional freefall, and suicidality emerges in the liminal space between unbearable suffering and uncontainable vulnerability.Healthcare professionals echoed this sense of depletion and ambivalence, observing that individuals often reach a point where the emotional resources to engage in recovery are simply absent. As one clinician described:Eventually people are like: fight with what? Because you can’t pour from an empty cup. (PT34, healthcare professional)This metaphor of the ‘empty cup’ speaks to the psychological exhaustion resulting from both living with the illness and trying to engage in recovery, which intensifies distress, at times to the point where life itself feels unmanageable. In such moments, suicidality may emerge as a reflection of the perceived impossibility of continuing without support, relief, or viable alternatives.The result is a painful tension of being caught between the chaos and exhaustion of the ED, and the uncharted, unsupported vulnerability of recovery. For some, this space felt unendurable. With no safe way forward and no tolerable way back, suicidality emerged not as a failure to cope, but as the only imaginable release from an impossible bind.
b‘Getting better feels worse’: recovery and isolationWhile recovery is often portrayed as a period of hope and progress, participants described it as a time marked by ‘feeling worse, not better’, due to experiences of deep isolation, grief, and disconnection, emotions which, for some, contributed to thoughts of suicide. In many accounts, the transition out of the ED was not experienced as liberation, but as a painful confrontation with everything the illness had taken away. As one participant notes below, this created a sense of exclusion and distance from others:[Friends] are having children, are in relationships, and you feel that you are behind and will never catch up. (PT32, healthcare professional)The ED had not just disrupted their present but had stolen their imagined future, leaving them stranded in a version of life that felt fundamentally disconnected from others. In this context, recovery could sharpen rather than soothe despair, sometimes reinforcing a sense that life was no longer liveable. Healthcare participants also observed this, describing how individuals often reached recovery only to be met with an absence of structure and meaning:You lose everything… friends, work… everyday life becomes so difficult… you start to feel hopeless. (PT38, healthcare professional)Hopelessness was not simply about current distress but about the perceived inability to rebuild a life that feels meaningful. Several participants described hitting clinical targets, such as weight restoration, while still feeling internally shattered.You hit your target weight and it’s like, oh, you need to maintain and live like this now. But you still feel like shit… and people start withdrawing support. (PT13, lived experience)This exemplifies how external indicators of progress can obscure internal suffering, leaving individuals with less support just as their emotional needs intensify. The withdrawal of care at this point may be unintentional, but it signals to participants that their struggle is no longer visible or valid, exacerbating feelings of disconnection and abandonment.Others described a pressure to appear ‘well’ to avoid disappointing others, even as they continued to feel overwhelmed.I feel that pressure of like: I’m managing things OK, but something has to give at some point… and I feel like not wanting to let other people down means that you’re probably more likely… to take it out [on yourself]. (PT10, lived experience)This highlights the emotional labour of recovery and the pressure to mask distress, to perform wellness, and to silence ongoing crisis. In this silence, suicidality can take root not as an impulsive response, but as the culmination of prolonged, invisible suffering. The experience of recovery, framed as a time of progress, instead becomes one of unspoken pain and lost potential.In this way, the data challenge simplistic narratives of recovery as linear or redemptive. Participants’ accounts instead reveal a complicated terrain in which recovery can deepen distress and even precipitate crisis, especially in the absence of adequate support, connection, and containment.
Theme 2—the outsider experience: feeling unseen, misunderstood, and burdensome
This theme explores how disconnection, shame, and marginalisation reinforce suicidal thoughts and stop help-seeking. The silence surrounding their experience of an ED and of suicidality resulted in an outsider experience that reinforced the belief that there was no space to express distress safely or authentically.
The two subthemes below exemplify these experiences and explore how suicidality was not only linked to the burden of the illness, but to the deeper existential pain of not being seen or understood.
aBeing ‘wrong’: when you don’t fit the script.The intersection of the ED with aspects of personal identity, such as gender, ethnicity, neurodivergence, and body size, was described by participants as compounding the complexity of the illness and contributing to key factors linked to higher suicidality. Individuals often found themselves measured against narrow narratives of what it means to have an ED, typically framed around young, thin, neurotypical, white, cisgender women with non-complex needs. Falling outside this template fostered a deep sense of unbelonging, where being overlooked and unseen led participants to feel that their suffering did not count, or worse, was not legitimate.Anorexia in particular is not a male diagnosis… I had to use the staff toilet because the unit didn’t have one for men… I think that there is something about my age and my gender and my diagnosis that doesn’t fit for a lot of people. (PT13, lived experience)When participants described how their experiences did not align with stereotypical ideas of what EDs should look like, particularly when their identities intersected with gender, race, neurodivergence, or body size, many felt invisible within clinical spaces and public discourse. This misalignment created not just practical barriers to support, but existential ones, reinforcing the sense that they were fundamentally out of place.While cultural and gender-based identities were central, several participants also identified neurodivergence, particularly autism, as a source of profound disconnection from both clinical systems and social norms. Many described being misunderstood or mischaracterised within services that were not attuned to neurodivergent communication or emotional processing styles.I do feel different to the average person, and I feel like I don’t fit in. And I do feel like my brain isn’t necessarily wired to deal with the world… I don’t really relate to the average, or the people that are around me. And I would say maybe that comes with an element of like suicidal risk. (PT06, lived experience)For neurodivergent individuals, suicidality was often intensified not only by heightened emotional sensitivity and social isolation, but by the ongoing experience of being ‘out of sync’ with the environments and systems meant to support them. This structural mismatch compounded feelings of erasure and reinforced a sense of being fundamentally ‘wrong’.For some, cultural and familial expectations further deepened this silence. One participant explained that their ethnic and cultural background made it impossible to talk to their family about their ED or suicidality, leaving them feeling isolated in both personal and professional contexts.I think like intersectional identity is like a big thing overall… my ethnic and cultural identity impacts a lot of things, my gender identity… that affects you, like me coming out [as non-binary], that’s quite a big deal. Because of my cultural background I can’t really do that right now and because I can’t do that, that’s made me feel very suicidal. (PT17, lived experience)This mismatch between lived reality and the ways EDs and mental health are culturally framed did more than exclude participants from support; it reinforced shame, silenced distress, and contributed to a fractured sense of identity and worth. For neurodivergent participants, this was often felt as a cumulative weight: not being seen, not being understood, and not being accommodated in either care settings or the wider world.For individuals with EDs, this repeated invalidation contributed to suicidality not simply as a symptom of distress, but as a response to being delegitimised and as a way of expressing or escaping a world in which one’s pain or identity is not allowed to exist. Thus, suicidality was not solely a reaction to ED symptoms, but a broader reflection of what it means to live as someone whose experience falls outside of what is culturally and clinically recognised as ‘real’, ‘deserving’, or ‘treatable’.
bThe weight of silence: when shame and stigma make suicide unspeakable.Participants described how suicidality was not only shaped by the ED itself, but by the painful reality that suicide was not only taboo, but in many cases something that was unspeakable, even within spaces meant to offer care. Suicidal thoughts were often described as ‘too much’ for others to hear, often evoking fear, discomfort, or panic. As a result, many individuals noted that the topic was highly silenced within society and services. This silencing contributed to a profound sense of alienation among individuals who felt unable to disclose their distress, reinforcing the perception that their experiences were both unwelcome and inexpressible within available relational or clinical contexts.We do find suicide very hard to talk about… it feels so uncomfortable people don’t know where to go, who to speak to, who to confide in. (PT28, lived experience)Participants described a culture of silence and stigma surrounding suicide, where simply naming it risked rejection or escalation. Many spoke of internalising this discomfort, learning to censor themselves, even in therapy. They feared being misunderstood, sectioned, or treated as unstable, and so their suicidality remained hidden, adding to the emotional and relational distance between themselves and others.If a clinician isn’t comfortable with the word suicide, how is the patient gonna feel comfortable bringing that to them? (PT01, lived experience)While many participants described how the stigma and silence surrounding suicide prevented them from seeking help, others reflected on how this silence shaped the way their suicidality was expressed. For some, their ED was consciously a more ‘socially acceptable’ means of ending their life as it was perceived as less shameful and less confronting for others than a direct or overt act of suicide.Anorexia was a more acceptable way to die… suicide was too hurtful to my mum. (PT05, lived experience)Even within treatment settings, participants reflected that suicidality was often not spoken about directly. Participants noticed that both those with lived experience and professionals would often substitute with softer language like ‘safety’ or ‘harm’. Although this softer language was at times preferred, it was felt to ultimately reinforce the perception that suicide was taboo and not something that could be addressed directly. This avoidance mirrored wider cultural messages that certain kinds of pain were simply too difficult to name or support.If you’re not used to dealing with acute care, dealing with suicide can be really, really overwhelming and so scary… when you say suicide, everyone goes into panic. (PT46, healthcare professional)In contrast, when suicide was named and space was created to share openly, participants described feeling less alone and more human when suicidality was treated as a part of the eating disorder experience rather than a threat to be contained. For some, the research interview itself was the first space where they could openly and truthfully share their experience of suicidality in a space where they felt not judged but understood.The combination of this silence and the secretive nature of EDs created a profound sense of isolation, reinforcing the belief that their suffering was not only misunderstood but unwelcome, and in some cases, increasing the risk of acting on suicidal thoughts.You’re keeping this massive, very burdening secret… you’re just very aware that it’s only on you and there’s no one that can help you with this. (PT23, lived experience)In this way, the silence around suicide did not conceal distress; instead, it amplified the sense of disconnection and otherness already experienced by people living with EDs. It reinforced the belief among individuals that they were too complicated, too intense, or too broken to be understood.
Theme 3—sparks of hope: protective factors against suicidality
While much of the data reflected distress and hopelessness, participants also described moments that helped them stay alive. These protective experiences were not limited to formal treatment; rather, they emerged through connection, purpose, and feeling believed. These protective moments did not erase the pain but instead offered something to hold onto.
a‘A reason to stay’: the grounding role of hope in suicidalityFor individuals with EDs, hope was not a constant or easily accessible. Suicidal thoughts frequently emerged when individuals felt there was no way forward, and in moments of deep entrapment, when life felt unchangeable and the pain of both the illness and the recovery process felt too much to bear. In these moments, having a spark of hope for the future was considered a significant protective factor against acting on suicidal thoughts for several participants.The power of hope when it comes to both the suicide and the eating disorder recovery is so key I think. (PT01, lived experience)As noted by some participants, it was often challenging to hold hope when in the depths of the ED or within treatment; therefore, having loved ones or clinicians who held hope during periods of darkness was experienced as lifesaving. Clinicians who expressed belief in the possibility of change or peers who offered compassion without conditions became lifelines during suicidal crises.I think patients need space and time to be able to know that someone is alongside them on this journey… you have to be with that journey with them, of trying to find even the little tiny chink of something… if someone’s talking to you, there is a tiny willingness, so then it’s a really important job… if you fail them then then they think the hope is gone. (PT48, healthcare professional)Participants described how hope was often introduced relationally through therapists, family members, or peers who gently affirmed that things could get better, even when the individual could not yet believe it themselves.There was a woman who’d been ill since she was seven, and when I told her I thought recovery was possible, she cried — no one had ever said that to her before. (PT01, lived experience)These moments of hope were not about just thinking positively; instead, they helped break the belief that things would never change, either with the ED or with suicidal thoughts. Hope served as a subtle but powerful resistance to the idea that death was the only escape and instead helped reintroduce the possibility of agency, change, and life beyond the illness and offered a reason to keep going.
b‘Finding purpose’: reconnecting with life outside the illness.As highlighted by both LE and clinician participants, for many participants, suicidality was shaped not only by emotional pain but by a deep sense of disconnection from themselves, from others, and from any future beyond the ED. As the illness ‘takes over your entire life’ and can ‘steal your identity, your purpose, and your future’, it was experienced as having gradually stripped away identity; for many, this made it hard to imagine a life that felt worth living. This hopelessness due to feeling that the ED had robbed them of their life and future was felt to be directly linked to increased feelings of suicidality.For some life doesn’t hold a lot of value anymore. When you are experiencing an eating disorder, that occupies a lot of your life, or you have had to put your life on hold. They haven’t been able to get the job they want. They have had to fall out of university. It is like where do they start… they feel that they are behind, and they will never catch up. (PT32, lived experience)Rebuilding an identity and future, thus addressing the losses caused by the ED, was felt to be a protective factor against acting on such suicidality. Looking beyond the existence that they were currently living and building a positive picture of what life without an ED could look like allowed people to build up reasons to stay alive. Seeing the self as more than just the ED, and seeing that it had not cost them everything, was seen to protect people and reignite a spark of hope for the future.I know there are a lot of triggers and stuff, but I think working, having a purpose, doing stuff in my community, and being social, they are all preventative factors. (PT20, lived experience)t’s about rebuilding that life, one that they are excited to return to. That’s one of the biggest protective factors. (PT31, healthcare professional)For many people with EDs, suicidality was experienced not only as a product of pain, but also of meaninglessness and loss. Reconnecting with a sense of purpose played an important role in reducing this despair. These small moments of purpose and reconnection with self, future, and others gave participants a sense that life could 1 day feel different. It was through these reconnections that some individuals found the hope and strength to keep going.
Theme 4—‘they only see weight’: how gaps in ED care reinforce isolation and risk
This theme explores how suicidality was shaped not only by the psychological distress of the ED itself, but also by how participants experienced support systems during times of crisis. Participants reflected on how certain aspects of care, such as limited accessibility, a focus on physical risk, or fragmented service pathways, could leave their suicidal distress overlooked. As a result, rather than alleviating risk, the absence or misalignment of support reinforced the very feelings of hopelessness and disconnection that contributed to suicidality.
The two subthemes below exemplify these experiences and explore how experiences of treatment or care systems are linked to increased suicidality for individuals.
a‘Overlooked and offloaded’: when suicidality is marginalised within eating disorder servicesAcross both lived experience and healthcare professional accounts, participants spoke of how suicidality was often sidelined within ED care. Whether overshadowed by physical risk or displaced by service boundaries, suicidal thoughts and self-harm were often treated as secondary concerns—either invisible, or someone else’s responsibility.For many, the prioritisation of physical health markers, particularly weight, meant that mental health risks like suicidality were downplayed or ignored altogether. While physical risk was recognised as urgent and life-threatening, participants felt this narrow focus came at the cost of acknowledging psychological distress.The only risk they see is weight; they don’t care otherwise. (PT16, lived experience)Suicide is often ignored or dismissed as a symptom of the anorexia, and that that will fix when you are recovered. It’s more complicated than that. (PT05, lived experience)This contributed to a sense of emotional abandonment. Requests for help around suicidality were met with silence, dismissal, or redirection, deepening participants’ sense of hopelessness and reinforcing the idea that their psychological pain was either not valid or too difficult to manage.If you’re brave enough to ask for help and then there’s nothing there, then it’s no wonder that people feel so hopeless and feel suicidal. (PT45, healthcare professional)These experiences were further compounded by the structural fragmentation of care. Many described how ED services narrowly addressed eating symptoms, while suicidality was seen as falling under the remit of general mental health teams. This often left people ‘pinged around’ or ‘batted back and forth’ between siloed services, with no team taking full ownership of their needs.They say they have suicidal thoughts, and then it’s like, oh no, they have to go to community mental health… but the eating disorders aren’t going to go away. (PT08, lived experience)Professionals recognised these dynamics too, acknowledging how limited resources, rigid service criteria, and diagnostic silos meant that suicidality was often seen as an ‘adjunct’ that is important but not within scope.There is nothing in the diagnostic criteria for anorexia or bulimia to mention suicidality… they must also be depressed, and that’s not our core business. (PT35, healthcare professional)As a result, suicidality was not only neglected but was actively displaced. Both staff and service users described feeling powerless within this system. For those in crisis, the repeated experience of being turned away or redirected reinforced a sense of invisibility and unworthiness. In this way, the fragmentation of care became part of the crisis itself, making help harder to access and distress even harder to hold.
b‘Sometimes help hurts’: when treatment experiences intensify suicide riskParticipants with lived experience of EDs acknowledged that treatment for these illnesses was often experienced as traumatic for some participants; such experiences within treatment settings contributed directly to suicidality. For some individuals, services were experienced as emotionally painful, invalidating, or traumatic. These experiences shaped not only how participants viewed their ED, but how they made sense of their own suicidality. This was due to the trauma of being rejected, delayed, or excluded from treatment. This was particularly salient for those with diagnoses like bulimia nervosa, binge eating disorder, or atypical anorexia.The assumption that you must be fine with your anorexia because you don’t look emaciated. I’ve had that said to me and that just compounds that I couldn’t possibly be sick enough, I don’t deserve support. All of that just beats you down. I think for me I was very much to the point of ‘I can’t get help, I would have to get a lot worse, but I can’t seem to get worse so what’s the point in carrying on?’ (PT04, lived experience)This feeling of being stuck, both within the illness and within a system that no longer held hope, leads to participants feeling psychologically cornered, intensifying suicidality as it increases the feelings of giving up due to the sense of futility around help-seeking as a result.For others, trauma occurred within the treatment setting itself. Inpatient environments, particularly during involuntary admissions, were described by many as restrictive, isolating, and emotionally overwhelming. While interventions like nasogastric feeding were acknowledged as medically necessary, they were often felt to be dehumanising when delivered under restraint or without adequate psychological support. Suicidality in these accounts was not separate from treatment but was a response to the experience of care that felt frightening, controlling, or inescapable.It was just the most traumatic thing ever… it was at that point I made several attempts on my life. (PT15, lived experience)Professionals echoed the concern, acknowledging that while clinically essential aspects of care and treatment could be experienced as traumatic and may inadvertently heighten suicide risk, this was particularly salient for individuals already struggling with a profound sense of powerlessness.Yes, it might be essential but are we paying enough attention to the unintended consequences?… ‘The only way to stop it is to actually end my life’ because they can’t see any better solution. (PT35, healthcare professional)While such restrictions were felt to be traumatic and triggered suicidal thoughts and behaviours, it was acknowledged that having care and support from staff was highly valued and was protective against acting on suicidality.He was phenomenal and validating… the impact a professional can have is huge. (PT01, lived experience)When clinicians offered care that was validating, human, and emotionally attuned and individuals felt like they were being taken seriously, seen as a whole person, and having hope held by others during times of despair was experienced as profoundly life-affirming.
Discussion
This study explored the inter-relationship between the experience of an ED and suicidality, with our findings highlighting the complexity of experiences faced by those with lived experience of ED. Overall, the findings highlight how suicidality in the context of EDs is shaped not only by the psychological and physical toll of the illness itself, but also by the emotional, relational, and systemic contexts in which individuals seek help. Participants described feeling trapped between the suffering of the disorder and the fear and uncertainty of recovery, while also experiencing a profound sense of disconnection and illegitimacy when their identities did not align with dominant ED stereotypes or when suicidality was silenced. Furthermore, interactions with care systems left many feeling unseen, unsupported, and at greater risk. However, moments of hope, feeling understood, and meaningful connection with others were described as powerful protective factors that helped people stay alive and engage in recovery. Across the findings, the theme of disrupted identity recurred, whether through the loss of the ED as a coping structure, the erasure of gender or neurodivergent identities in care, or the sense of life being permanently ‘off track’. These disruptions did not merely cause distress but underpinned the emergence of suicidality by stripping individuals of coherence, belonging, and future orientation. Furthermore, participants’ accounts of being unable to speak about suicidality, even within care, highlight the role of cultural and systemic silence in compounding risk. Suicide, in this context, was not simply a response to individual pain, but also to the absence of space in which that pain could be acknowledged and held.
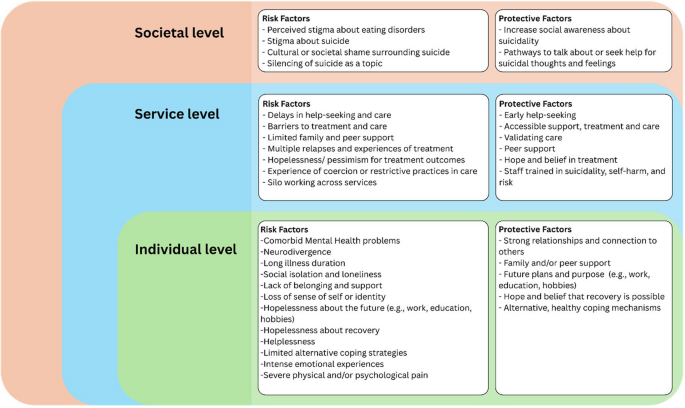
Figure 2 exemplifies the key factors noted within these themes across Bronfenbrenner’s ecological systems [25] in which the risk of suicide is emphasised not only at the individual level, but also as stemming from systemic and societal factors, denoting the complex interplay of issues when considering the risks facing those with EDs.
Fig. 2
These findings highlight important elements of suicide risk within existing theories of suicidality, namely the IPTS [13] with increased helplessness, hopelessness, and burdensomeness arising as key elements of suicide risk experienced by people with EDs. Furthermore, our findings highlight that individuals with EDs have high levels of acquired capability of suicide [13] due to the elevated physical pain tolerance directly linked to illness symptoms and the physical nature of the illness. Additionally, some participants in this study described using their ED as a form of slow suicide, viewing it as a less stigmatised way to die. For some, death from an ED was perceived as inviting less blame or guilt for loved ones compared to suicide. These insights highlight the complexity and unique challenges surrounding suicidality among individuals with EDs. These findings provide an understanding of why people with these illnesses are at risk of suicide as their experiences align closely with pre-existing theories of suicide risk.
Our findings, however, add to this theoretical understanding by considering that these risk factors are active and constantly evolving and, thus, do not map neatly onto a particular point in one’s journey. Likewise, these findings indicate that there are various risk periods (e.g. during recovery, when treatment is intensified); thus, personal risk is likely to vary depending on the individual, the period of their journey, and how a range of factors interact. This builds a complex picture, which needs to consider a range of multifaceted and intersecting biological, sociocultural, and psychological factors (e.g. emotional and interoceptive deficits) that may contribute to suicide risk among individuals with EDs. While elements of the IPTS such as helplessness, hopelessness, and burdensomeness may explain underlying feelings linked to feeling suicidal, it is important to see these within the context of the ED experience to fully understand how the illness directly impacts on one’s suicidality. These findings highlight that the ED experience in and of itself creates a push–pull effect in which individuals note that the illness is debilitating and has a negative impact that increases feelings of suicidality, but also that the process of recovery from the disorder, and loss of it as a coping mechanism, potentially creates increased suicidality. This conflict of being unable to live with the illness but also without it highlights the unique challenge facing those with living experience of an ED when considering risk of suicide. Furthermore, these findings highlight that intersecting identities and co-occurring mental health problems add to the complexity facing individuals with EDs as these aspects compound feelings of suicidality and thus increase the risk of engaging in suicidal behaviours. These findings are supported by a recent study which highlights that conventional risk factors for suicide, such as those noted in some existing models (e.g. IPTS), might be less important in those with EDs than factors related to clinical complexity; for instance, self-harm and co-occurring conditions [26]. Given the limitations of these models, efforts are being made to develop less focused theories of suicidality that move beyond psychiatric categories to ensure that we are able to further understand the causes of suicide risk, including the development and refinement of the Integrated Motivational-Volitional (IMV) Model of Suicidal Behaviour [27]. To date, the IMV has not been tested with ED populations; however, given the overlapping themes, these findings support the use of the IMV model of suicide to explore suicide risk among people with EDs [27, 28]. Across the themes, suicidal thoughts were shown to be shaped not only by emotional pain but also by a deep sense of entrapment leaving them with no way out. This reflects the IMV model’s view of entrapment as a central driver of suicidal ideation. In addition, disconnection, shame, and marginalisation were experienced, which reflect the model’s emphasis on experiences of defeat, humiliation, and being a burden to others. These factors were often intensified by treatment environments that failed to acknowledge emotional distress, leading some to feel they were beyond help. Furthermore, these findings identified protective factors that helped disrupt this process, including the protective role of connection, purpose, and hope. These align with the IMV model’s recognition of protective factors that can reduce the risk of suicidal behaviour, offering important insight into what may interrupt this trajectory for people with EDs [27]. Future theoretical and clinical frameworks must recognise the unique and layered mechanisms of suicidality in EDs, rooted not only in psychopathology but also in social exclusion, identity disruption, and system-level silencing.
Alongside these risks at an individual level, our findings highlight how these exist within the wider context of both treatment or services, and culture and society. Where individuals with EDs experienced suicidal thoughts and behaviours, there were often high levels of shame and secrecy related to this aspect of their journey due to the lack of acceptance of the topic within the ED community and services, and within wider society. The separation of EDs and suicidality within care was noted within this study as adding to the silence around this topic and the view that suicide and EDs are separate issues. Our findings, however, indicate that suicide is a key issue linked to EDs; therefore, there is a need for ED clinicians to be more confident to talk about suicide and bring this topic into treatment, rather than referring patients on to other services when faced with suicide risk.
While these findings help to understand why people with EDs are at risk of suicide, our themes also help to identify the countering protective factors and reasons why participants had stayed alive and persevered with recovery even when it is difficult. Knowing why people may give up hope, or want to die, can help us utilise these protective factors to develop individualised, preventative approaches to suicide. Our findings note the importance of hope, support, and purpose, as well as highlighting the role of peer support and hearing hopeful recovery stories from others with lived experience as a means to hold hope that recovery is possible. Having clinicians holding hope and providing ongoing support and care has been highlighted in previous literature as salient, particularly considering controversial discussions regarding longstanding, complex EDs and palliative care pathways for EDs [29, 30]. We believe that treatment and care can adapt to tackle these challenges by exploring the experiences of suicidality with those with lived experience of EDs.
Strengths and limitations
To our knowledge, this is the first qualitative study to explore the inter-relationship between the experience of an ED and suicidality. As such, it makes a novel contribution to the field by offering in-depth, interpretive insights into the psychological processes underlying this association. A key strength of the study is the richness and depth of the data, drawn from a diverse range of participants in terms of clinical experience, age, and professional background. This allowed for the development of nuanced themes that cross diagnostic and experiential boundaries, capturing shared challenges as well as individual variation.
However, several limitations should be acknowledged. While the diversity of participant experiences was a strength, the sample lacked ethnic diversity, with the majority identifying as White. Few participants were from South Asian, Black, or Mixed ethnic backgrounds. Given that cultural factors were identified in the data as influencing both ED and suicidality experiences, future research should prioritise the inclusion of underrepresented groups. This could be achieved through targeted recruitment strategies, including collaboration with community organisations, multilingual materials, and culturally sensitive outreach methods.
The study also used a self-selection recruitment strategy, which may have introduced bias towards participants who already perceive suicidality as a significant issue within the ED population. This may have limited the range of views captured and reduced the representation of individuals who do not frame their experience through a suicidality lens. Furthermore, voices from key groups such as those with long-standing EDs, older adults, men and boys, and gender-diverse individuals were underrepresented. Future research should centre these perspectives to build a more inclusive and comprehensive understanding of suicide risk in the context of EDs, particularly with attention to how chronicity, identity, and hopelessness intersect.
Given the interpretive nature of the analysis, these findings are shaped by the researchers’ positionality and theoretical lens. Without participant validation (e.g. member checking), there is a risk that some nuances of participant meaning may have been unintentionally reframed or overlooked. However, this is consistent with the reflexive thematic analysis approach, which embraces researcher interpretation as a necessary and transparent part of meaning-making.
Conclusions
Our findings underscore the complex and multifaceted relationship between EDs and suicidality. By foregrounding the real-world perspectives of individuals with lived and living experience of EDs, alongside clinicians who support them, this study begins to unravel the underlying reasons why people with these illnesses may experience suicidality. These insights can support treatment and care approaches that not only address suicidality directly but also account for the persistent risk of suicide that may emerge at different stages of recovery.
Importantly, our findings highlight the need for ED treatments to be person-centred and responsive to the concerns raised by individuals themselves, rather than solely focusing on symptom reduction. The complexity of ED experiences calls for flexible, individualised care that is embedded within a structured, evidence-based treatment framework. This approach may be better equipped to engage individuals and address the psychological factors contributing to suicidality.
Finally, this study advances our understanding of suicidality in the context of EDs by identifying psychological processes and risk mechanisms not currently accounted for within existing theoretical models. As such, these findings offer early evidence to support the development of a new, ED-informed theory of suicidality, shaped by the voices of those with lived experience.