

By
and
#SeattleTimes staff
![]()
The #MentalHealthProject is a #SeattleTimes initiative focused on covering #mental and #behavioralhealthissues. It is funded by Ballmer Group, a national organization focused on economic mobility for #children and families. The #SeattleTimes maintains editorial control over work produced by this team.
Navigating the #mentalhealthsystem can mean sorting through a tangled web of confusing diagnoses, frustrating conversations with insurers, and varying levels of care at private and public #health care agencies.
But unless you’ve gone through it yourself or have helped a loved one who needs care, it’s hard to visualize the bureaucratic hoops someone has to jump through, or see the full picture of the strained, complicated system at large.
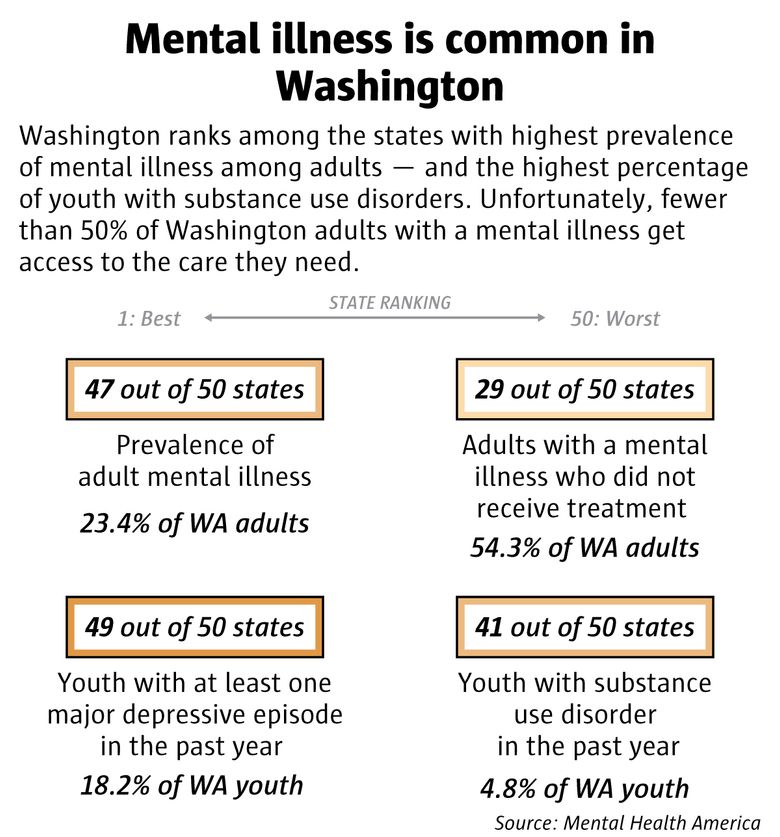
Many people have personal or family experience with #mentalillness — about 1 in 5, or 1 million #Washington #adults, have a diagnosable #mentalhealthcondition. You, your neighbors, friends, colleagues and family members are affected by #mentalillness. The #COVID-19 #pandemic has made everything harder, as people face economic and social uncertainty on top of concerns for their health. Backlogs for care keep growing as systems are stressed beyond capacity.
Everyone’s situations will vary: Individual circumstances like whether or not a person has access to financial resources or support from family or friends can play huge roles in determining a person’s path, and it’s impossible to chart all outcomes. But the data below, along with examples of how the system’s constraints play out in the real world, aims to give some of the broad strokes of what Washington’s #mentalhealthcare landscape looks like.
Access to #mentalhealthcare
The #SeattleTimes’ #MentalHealthProject has been exploring issues of access to #mentalhealthcare. A series of stories published in December took a deeper look at why it’s so hard to get help when you need it.
Why it’s so hard to find a #therapist, and stories from readers
Naomi Ishisaka: Finding care shouldn’t be this hard
Guide: What to know when looking for therapy
How Washington’s approach to #mentalhealth has changed
Mapping #mentalhealth: Washington’s capacity for care
Guide: Tips for when you can’t find a #therapist
#JamesDonaldson notes:
Welcome to the “next chapter” of my life… being a voice and an advocate for #mentalhealthawarenessandsuicideprevention, especially pertaining to our younger generation of students and student-athletes.
Getting men to speak up and reach out for help and assistance is one of my passions. Us men need to not suffer in silence or drown our sorrows in alcohol, hang out at bars and strip joints, or get involved with drug use.
Having gone through a recent bout of #depression and #suicidalthoughts myself, I realize now, that I can make a huge difference in the lives of so many by sharing my story, and by sharing various resources I come across as I work in this space. #http://bit.ly/JamesMentalHealthArticle
How do people navigate the #mentalhealthsystem?
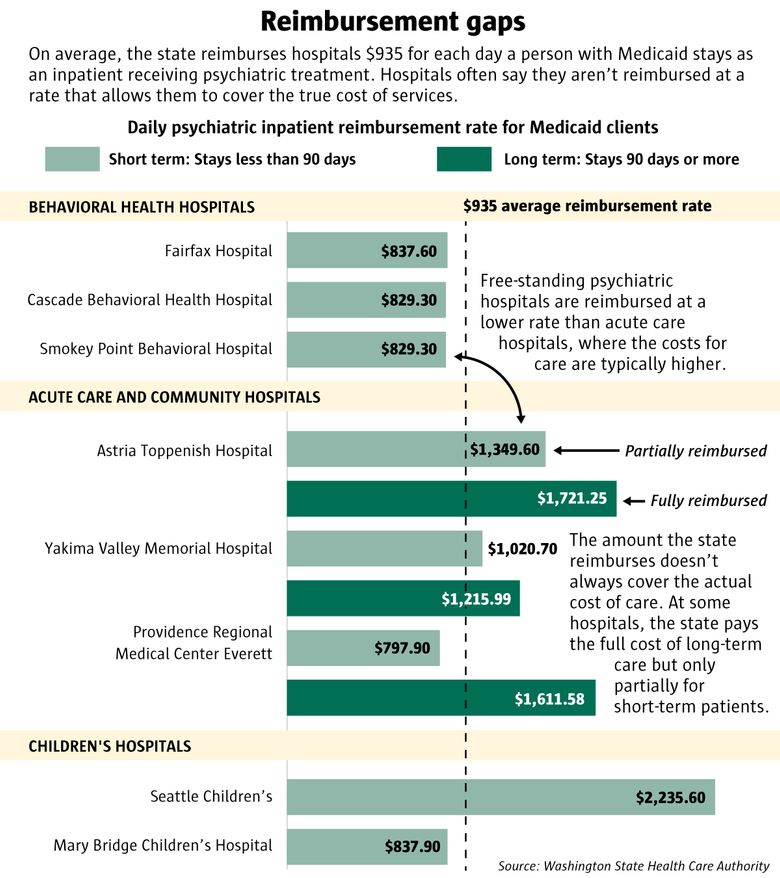
The #mentalhealth landscape is really multiple systems spanning #behavioralhealth, hospitals, jails and correctional facilities, all under the jurisdiction of different county, state and federal agencies. The following charts explain what happens for people seeking care in both urgent and non-urgent settings.
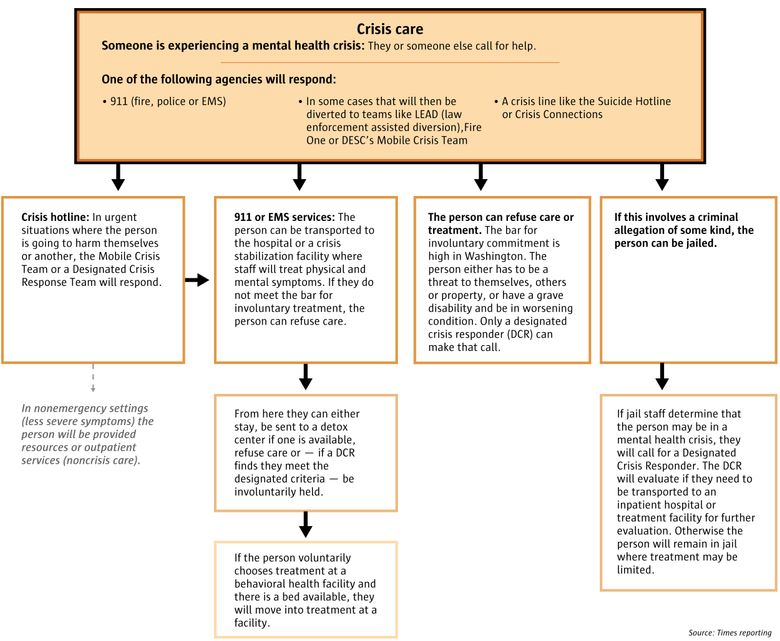
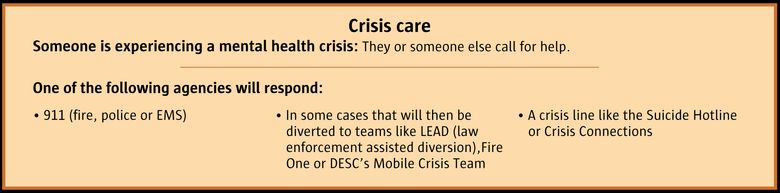
WALK THROUGH THE STEPS OF CRISIS CARE
?
Crisis hotline: In urgent situations where the person is going to harm themselves or another, the Mobile Crisis Team or a Designated Crisis Response Team will respond.
In nonemergency settings (less severe symptoms) the person will be provided resources or outpatient services (noncrisis care).
?
911 or EMS services: The person can be transported to the hospital or a crisis stabilization facility where staff will treat physical and mental symptoms. If they do not meet the bar for involuntary treatment, the person can refuse care.
?
From here they can either stay, be sent to a detox center if one is available, refuse care or — if a DCR finds they meet the designated criteria — be involuntarily held.
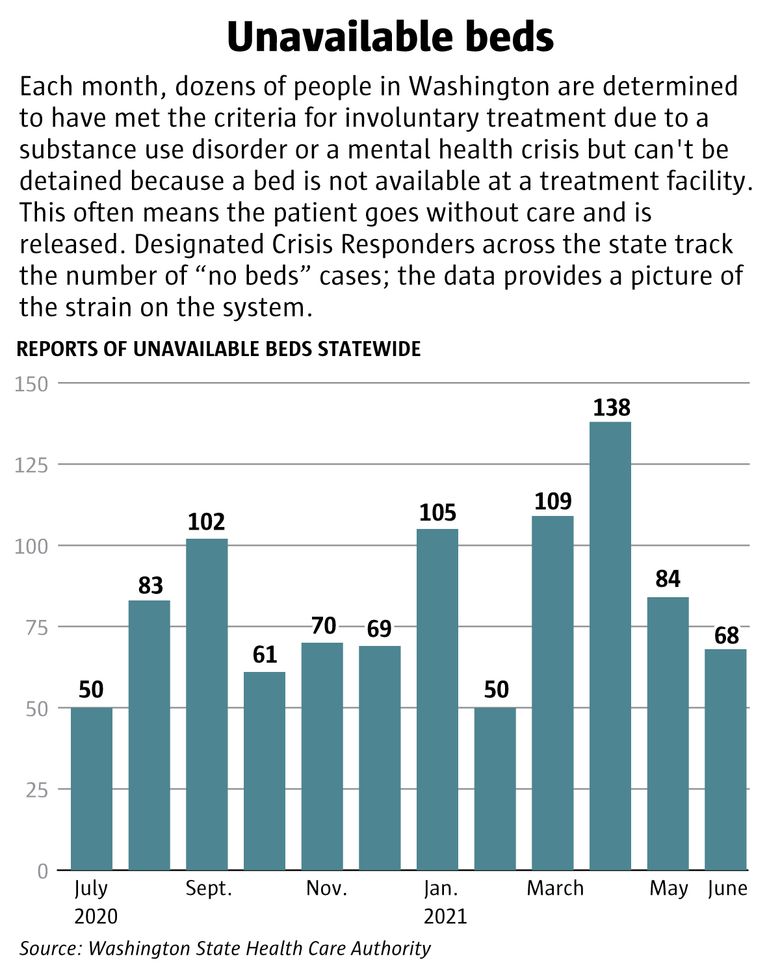
How it plays out: You are having a #mentalhealthcrisis and a friend calls 911 to get help. A designated crisis responder finds that you are a danger to yourself and getting worse, meaning you meet the bar to be involuntarily committed to a facility. But staff can’t find a bed at a #psychiatric treatment center and the emergency room that you were brought to cannot keep you overnight either — they are not properly equipped to provide longer term care and besides, the ER is loud and makes your symptoms worse. The DCR makes a note but you are ultimately released in order to avoid boarding you at a hospital. Your family is in another state and can’t pick you up. You are released and you go home alone.
?
If the person voluntarily chooses treatment at a #behavioralhealth facility and there is a bed available, they will move into treatment at a facility.
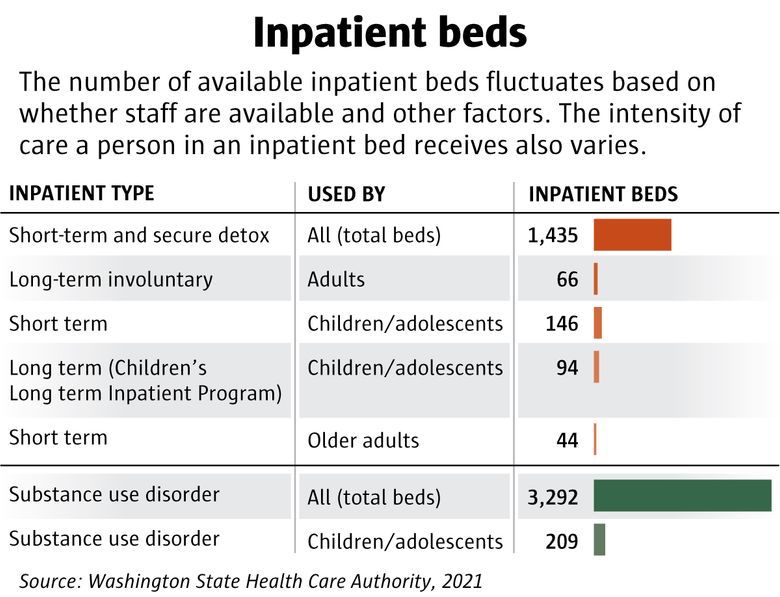
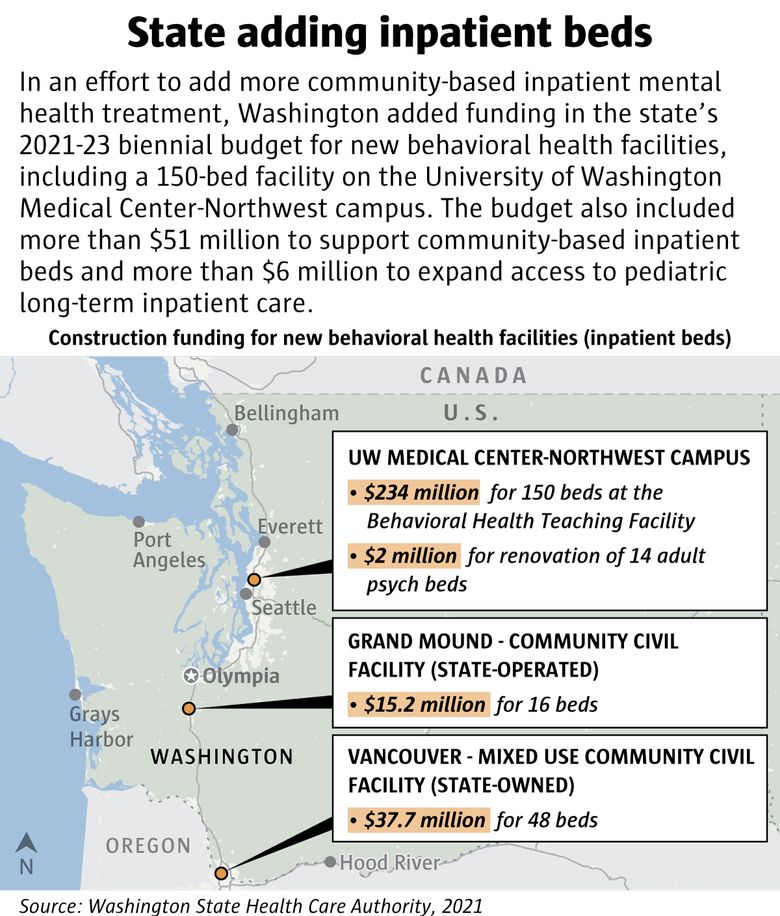
How it plays out: You’re the head of a #behavioralhealth agency and are concerned about a persistent lack of inpatient beds for people in #mentalhealthcrisis. You’d like to add beds to your existing 16-bed facility. But it won’t be easy. A federal law prohibits agencies from getting reimbursed through Medicaid if they have more than 16 beds (for most age groups). The law was part of the nation’s move away from institutionalization — but in practice, it means you’ll have to jump through lots of logistical hoops to add more beds. One of your only options is to build a new facility. Once you locate a building site, you have to apply for building permits through your local jurisdiction, pursue licenses through the state’s health department, build the building, hire staff and negotiate with public insurance providers. The process, from start to finish, can take years.
______________
CONTINUING FROM SOMEONE CALLING FOR HELP
?
The person can refuse care or treatment. The bar for involuntary commitment is high in #Washington. The person either has to be a threat to themselves, others or property, or have a grave disability and be in worsening condition. Only a designated crisis responder (DCR) can make that call.
______________
CONTINUING FROM SOMEONE CALLING FOR HELP
?
If this involves a criminal allegation of some kind, the person can be jailed.
?
If jail staff determine that the person may be in a #mentalhealthcrisis, they will call for a Designated Crisis Responder. The DCR will evaluate if they need to be transported to an inpatient hospital or treatment facility for further evaluation. Otherwise the person will remain in jail where treatment may be limited.
______________
Navigating noncrisis #mentalhealthcare
The path to finding a #therapist or getting a prescription to ease symptoms related to #mentalillness often starts in a primary care physician’s office or at a community-based health center. Your insurance can determine what kinds of care are most accessible to you.
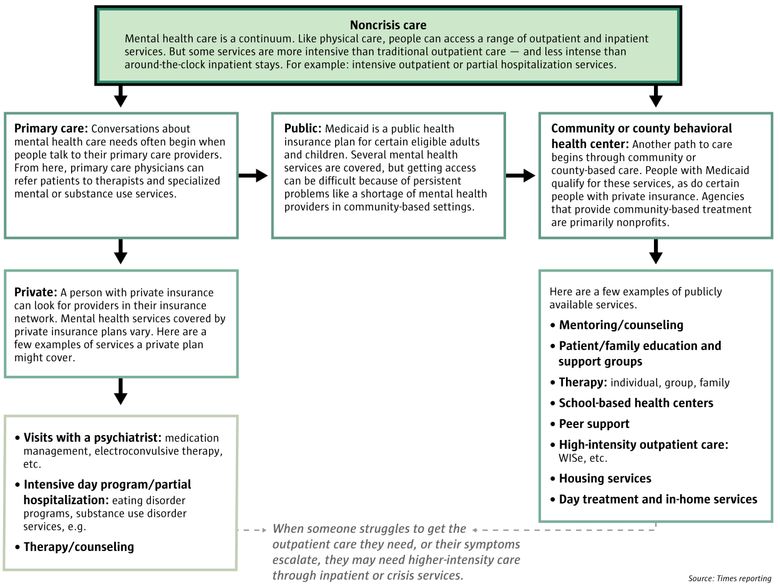
WALK THROUGH THE STEPS OF NONCRISIS CARE
After people leave inpatient care, they might be referred to less intensive services, such as partial hospitalization programs or outpatient therapy.
?
Primary care: Conversations about #mentalhealthcare needs often begin when people talk to their primary care providers. From here, primary care #physicians can refer #patients to #therapists and specialized mental or substance use services.
?
Private: A person with private insurance can look for providers in their insurance network. #Mentalhealthservices covered by private insurance plans vary. Here are a few examples of services a private plan might cover.
?
• Visits with a #psychiatrist: medication management, electroconvulsive therapy, etc.
• Intensive day program/partial hospitalization: eating disorder programs, substance use disorder services, e.g.
• Therapy/counseling
______________
CONTINUING FROM PRIMARY CARE
?
Public: #Medicaid is a public health insurance plan for certain eligible #adults and #children. Several #mentalhealthservices are covered, but getting access can be difficult because of persistent problems like a shortage of #mentalhealthproviders in community-based settings.
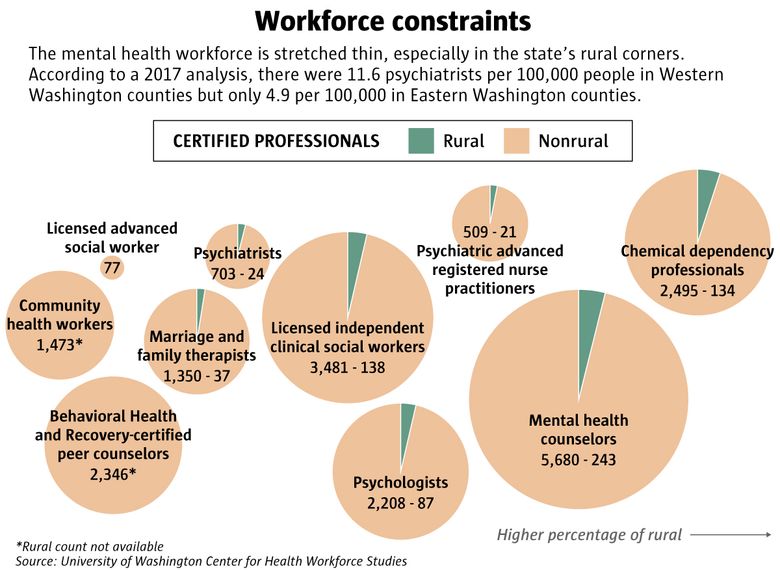
How it plays out: You’re starting to experience more serious symptoms of #depression and #anxiety, and feel like you might need more intense care than weekly sessions with your #therapist. Last week, your primary care provider decided you’d benefit from seeing a #psychiatrist, who could evaluate you for a range of conditions and possibly prescribe medication. But the #psychiatrist they’d like you to see is booked out at least three months. A shortage of #psychiatrists and other #mentalhealthproviders means many folks can’t get timely appointments. Only 727 #psychiatrists are credentialed to work in #Washington.
______________
CONTINUING FROM PRIMARY CARE OR PUBLIC
??
Community or county #behavioralhealth center: Another path to care begins through community or county-based care. People with #Medicaid qualify for these services, as do certain people with private insurance. Agencies that provide community-based treatment are primarily nonprofits.
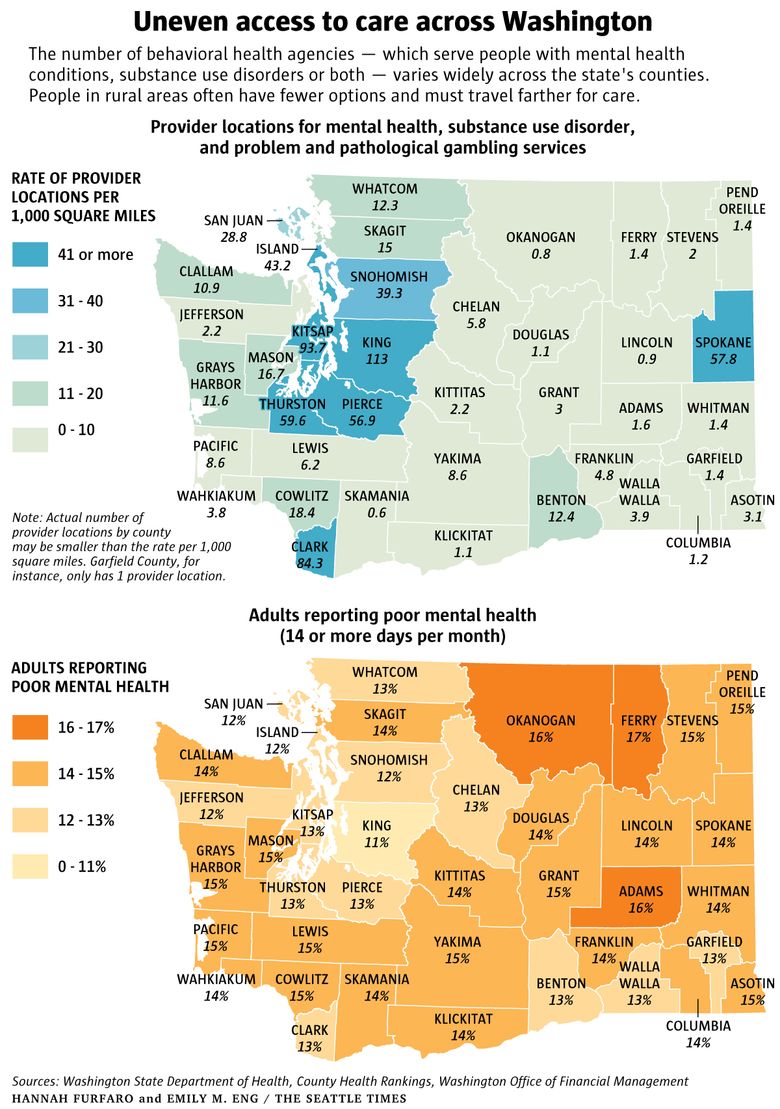
How it plays out: You’ve felt the weight of the #pandemic for months now, and find that daily life — work, chores, even spending time with friends and family — feels less rewarding than it used to. You’re waking up at odd hours and can’t focus at work. You’d like to schedule an appointment with a #therapist to talk about your symptoms; you’re worried you might be experiencing #depression. But you live in Garfield County in southeastern #Washington, one of several rural corners in the state where it can feel impossible to find a #mentalhealthprovider. In 2020, only one #mentalhealthprofessional served your county. You give them a call, but they don’t take your insurance, and plus, they’re not taking any new clients.
?
Here are a few examples of publicly available services.
• #Mentoring/#counseling
• #Patient/family education and support groups
• Therapy: individual, group, family
• School-based health centers
• Peer support
• High-intensity outpatient care: WISe, etc.
• Housing services
• Day treatment and in-home services
Emily M. Eng: 206-515-5636 or eeng@seattletimes.com; on Twitter: @Emily_M_Eng. Emily Eng is a graphic artist at The #SeattleTimes.
Hannah Furfaro: hfurfaro@seattletimes.com; on #Twitter: @HannahFurfaro. Hannah Furfaro is a #mentalhealthreporter at The #SeattleTimes. She has a master’s degree in science and health journalism from Columbia University, and wrote about neuroscience and psychiatry before joining The Times. She previously published stories in Science, The Wall Street Journal and The Atlantic, among other places. Send her tips at hfurfaro@seattletimes.com or find her on Twitter @hannahfurfaro.
Esmy Jimenez: 206-305-4872 or ejimenez@seattletimes.com; on Twitter: @esmyjimenez. Esmy Jimenez is a reporter covering #mentalhealth for The #SeattleTimes.


